Whereas this site mainly focuses on masculinity-femininity as it pertains to beauty in women, it is also interested in promoting overall high aesthetic standards among female models and beauty pageant contestants. This post addresses some anthropological data on the proportions of a beautiful backside in white women, pertaining to both masculinity-femininity and other aspects; data on non-white women were not available at the time of this posting. The data shown below can be used to describe with some precision why the backsides of high-fashion models are typically seen as unattractive, even pathetic, by most people, with the notable exception of gay fashion designers.
The report below was written by Ramon Cuenca-Guerra and Jorge Quezada, and was published online by the journal Aesthetic Plastic Surgery on Oct 26, 2004. Beautification of the buttocks often requires liposuction (removing excess fat tissue in a given region).
What Makes Buttocks Beautiful? A Review and Classification of the Determinants of Gluteal Beauty and the Surgical Techniques to Achieve Them
Abstract
Background: No reports can be found in medical literature describing the anatomic details that make the buttocks beautiful, nor the defects in this region that can help the surgeon decide whether gluteal prostheses are necessary or not, and, if so, which type, design, and volume of prostheses should be used, in which plane they should be placed, and so forth.
Methods: The authors studied 1,320 photographs of nude women and measured 132 female patients ages 16 to 62 years. They found that four characteristics determine attractive buttocks. They also found the balanced anatomic dimension of the maximal gluteal projection.
Results: On the basis of the information obtained, the defects of the gluteal region were classified into five types, resulting in surgical recommendations intended to achieve buttocks as close as possible to the standard of beauty, with the right volume and projection.
Conclusions: The authors concluded that surgery for correction of the buttocks involves more than projection and volume. The surgeon must be familiar with the signs of beauty so an attempt can be made to recreate them. Most importantly, the surgeon should achieve buttocks with projection and volume. However, these must be in a balanced proportion with the rest of the body.
Keywords: Buttocks, Aesthetic surgery, Gluteal implants, Gluteal prosthesis, Gluteoplasty.
Presented at the XIV International Congress of FILACP Cancun, Mexico, 2002.
Introduction
The buttocks are an important element of sexual attraction, occupying a major place in the concept of beauty recognized by most cultures and ethnic groups. Consequently, for several decades, a number of surgeons have been attempting to correct alterations in the shape and volume of this region by resection and skin adjustments, placement of gluteal prostheses, liposuction and lipoinjection, or other techniques. To date, however, no anthropometric studies and/or aesthetic analyses of the gluteal region are available that indicate what signs of beauty should be spared or recreated, the extent to which projection or volume should be increased, and the harmonic proportion that should exist between this region and the rest of the body.
Recognizing this, and aiming to make teaching easier in our postgraduate course, we decided to discover what characteristics or details make buttocks attractive, and to determine the ideal posteroanterior projection for each body archetype. Once we had this information, we set out to divide the various alterations in the gluteal region into groups, so as to establish criteria and determine the surgical techniques for correcting each set of defects and sculpturing the details that mark the difference between attractive buttocks and those with projection and volume but with no harmony.
Materials and Methods
Aesthetic Analysis of the Gluteal Region
To discover which anatomic features make the gluteal region attractive and seductive, we studied 2,400 photographs of nude women ages 20 to 35 years, as seen from behind, in different postures and actions, and from different periods (1954 through 2001), to identify each of the features and anatomic elements that create harmony and beauty. The final analysis included 1,320 photographs in which the gluteal region was seen full from behind, in three-quarter profile from behind, and in full profile. Also, the photographs showed subjects standing up or lying face down and in full extension or slight flexion - no more than 15° - while walking. The selected photographs were analyzed by six certified plastic surgeons, who pointed out which buttocks they considered attractive and harmonious, and features on which this attractiveness depended.
Anthropometric Analysis of the Gluteal Projection
We considered that the most attractive feature of the gluteal region is anteroposterior projection. However, to determine the ideal projection, fixed landmarks that were easily identifiable, either visually or by palpation, had to be established. These were determined to be the greater trochanter (point A), the point of maximal projection of the mons veneris (point B), the point of maximal gluteal projection (point C) and the anterior superior iliac spine (point D). Once these anatomic landmarks were established, we drew a vertical line through point A, which is the body's gravity line (axis of balance) [4], a second parallel line through points D and B, and a third horizontal line through points C, A, and B perpendicular to the other two and equivalent to that described by Gonzalez-Ulloa [2] in 1979. This gave us the ideal plane of maximal gluteal projection (Fig. 1). With all these parameters in mind, we set out to apply them to 132 women 16 to 62 years of age, 155 to 170 cm in height, and no more than 5 kg overweight.
(Note: All images below can be clicked for larger versions.)
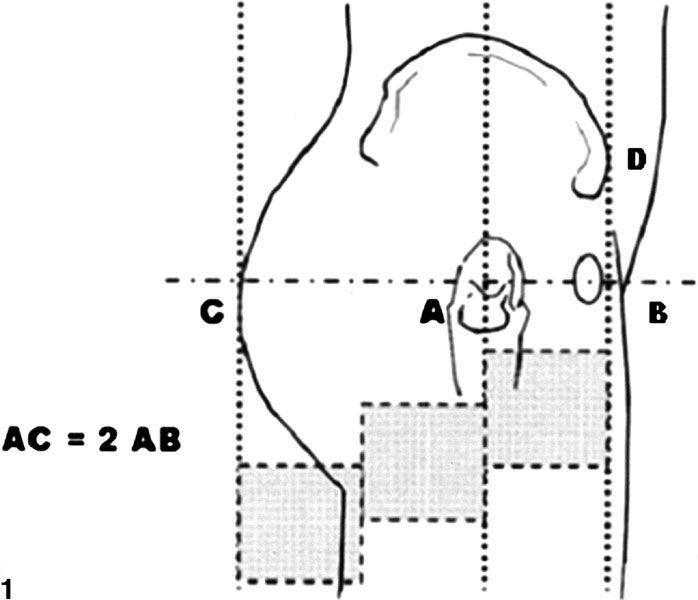
Figure 1. (A) Greater trochanter, (B) Point of maximal projection of the mons veneris, (C) Point of maximal gluteal projection, (D) Anterior superior iliac spine. The CB line points to the maximal ideal projection of the buttocks. The ideal proportion is a 2:1 ratio between AB and AC.
Results
Aesthetic Analysis of the Gluteal Region
The analysis performed on the 1,320 photographs highlighted four features that were considered consistent features of beauty, as determined by several anatomic structures of the gluteal region. These four characteristics may appear together or independently of each other (Fig. 2):
- Lateral depression. This hollow on the lateral aspect of each buttock is formed in its deepest point by the greater trochanter, superiorly by the insertion and belly of the gluteus medius, inferiorly by the insertion of the vastus lateralis, and posteriorly by the insertion of the quadratus femoris, with the belly of the gluteus maximus over the latter.
- Infragluteal fold. This horizontal crease is under the ischial tuberosity. Its inferior border is formed by the insertions of the semitendinous muscle and the long belly of the biceps femoris in the ischial tuberosity. Superiorly, it is formed by the lower border of the gluteus maximus. It arises in the median gluteal crease and follows a lateral curve, with a proximal concavity, no further than the union of the semitendinous muscle with the biceps femoris.
- Supragluteal fossettes. These are two hollows located on either side of the medial sacral crest. They are formed in their deepest part by the posterior superior iliac spine and medially by the multifidus muscle. In a more superficial plane, they are bounded by the lumbodorsal aponeurosis, and inferiorly and laterally by the insertion of the gluteus maximus.
- V-shaped crease. In 45% of the photographs, this crease was observed, formed by two lines arising in the proximal portion of the gluteal crease. Directed toward the supragluteal fossettes, these lines are formed by the insertion of the gluteus maximus in the lumbodorsal aponeurosis. They measure no more than one-third of the distance between the gluteal crease and the supragluteal fossettes.
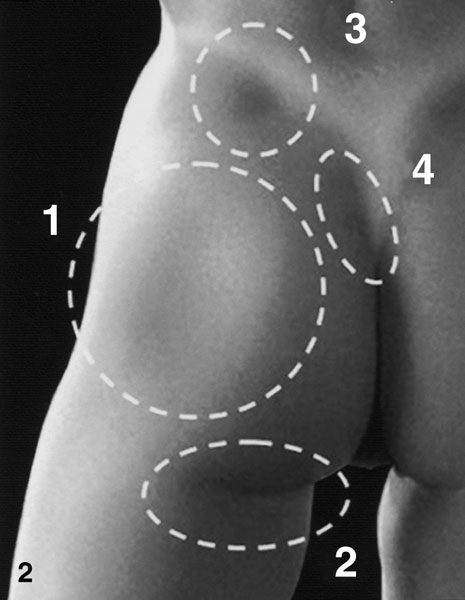
Figure 2. Consistent features of beautiful buttocks: (1) Lateral depression, formed by the lateral border of the gluteus maximus, the quadratus femoris, and the insertions of the gluteus medius and vastus lateralis to the greater trochanter, (2) Infragluteal fold, created by the ischial tuberosity, the insertions of the semitendinous muscle and long belly of the biceps femoris, and the lower border of the gluteus maximus, (3) Supragluteal fossettes (one on either side) over the posterior superior iliac spine, created by the multifidus muscle, the lumbodorsal aponeurosis, and the insertion of the gluteus maximus, (4) V-shaped crease, arising in the proximal portion of the gluteal crease.
An additional feature that may contribute to beautiful buttocks is lumbar hyperlordosis. This hyperextension of the spine in the lumbosacral region is an ethnic feature (i.e., in black or mulatto persons), and sometimes is the result of a forced posture since childhood. In these cases, the sacrum is horizontalized an average of 5° to 7°, which in a side view gives the impression of a greater buttocks projection than the actual one, normally produced by the muscles in this region.
Anthropometric Analysis of the Gluteal Projection
An examination of points A, B, and C as well as the vertical lines crossing them in 32 women with height and weight as described in the Materials and Methods section, and with an attractive gluteal projection showed that the distance between points A and B is equal to half the distance between points A and C, which gives a 2:1 ratio (Fig. 1).
The same measurements for 100 patients who requested gluteal increase showed that 27 apparently had no gluteal projection, although they maintained the 2:1 ratio in the A-C and A-B distances. This was attributable to an excess of lumbar, supragluteal, and subgluteal fat tissue, which concealed the actual gluteal projection. In this same group of patients, 35 women stated their request for more projection in this area while expressing satisfaction with the volume, once the measurements were completed, it became evident that the ratio of the distances A-C and A-B was lower than 2:1, it usually was 1.5:1, and 30% of the patients were found to have paralumbar and subgluteal lipodystrophy. In 19 patients, there seemed to be adequate gluteal projection; however, examination showed a lack of volume and horizontalization of the sacrum (hyperlordosis) as well as a 2:1 or slightly lower ratio. Furthermore, 13 women with an ideal or lower-than-ideal weight were found to have a lack of volume and projection, with a ratio below 2:1. Finally, six patients older than 55 years showed signs of aging in the gluteal region such as hypotrophy of the skin, fat, and muscles as well as ptosis of the tissues in the area.
For didactic purposes, we divided these results into five categories of women:
Type 1. Women with a 2:1 or higher ratio, adequate volume, and good projection, but with an excess of supragluteal, paralumbar, and subgluteal fat (Fig. 3).
Type 2. Women with a ratio lower than 2:1 who have enough volume and laterolateral projection, but little anteroposterior projection. Thus, these women have an appearance of wide hips with relatively flat buttocks. Usually, they also have an excess of supra- and subgluteal tissue (Fig. 4).
Type 3. Women with lumbosacral hyperlordosis, usually with a ratio of 2:1 or slightly lower. The horizontalization of the sacrum gives the appearance of a large anteroposterior projection. However, these women lack volume and side-to-side projection, and sometimes there is an excess of subgluteal fat (Fig. 5).
Type 4. Usually sportswomen, very thin or at their ideal weight, with no excess fat and with a lack of volume and gluteal muscle mass projection which leads to an android (cylindrical) pelvis. This category includes women with a ratio lower than 2:1 and with lack of both projection and volume. Occasionally, there may be some excess subgluteal fat (Fig. 6).
Type 5. Women with senile buttocks, as evidenced by hypotrophy of skin, fat, and muscle as well as ptosis of tissues in the area (Fig. 7).
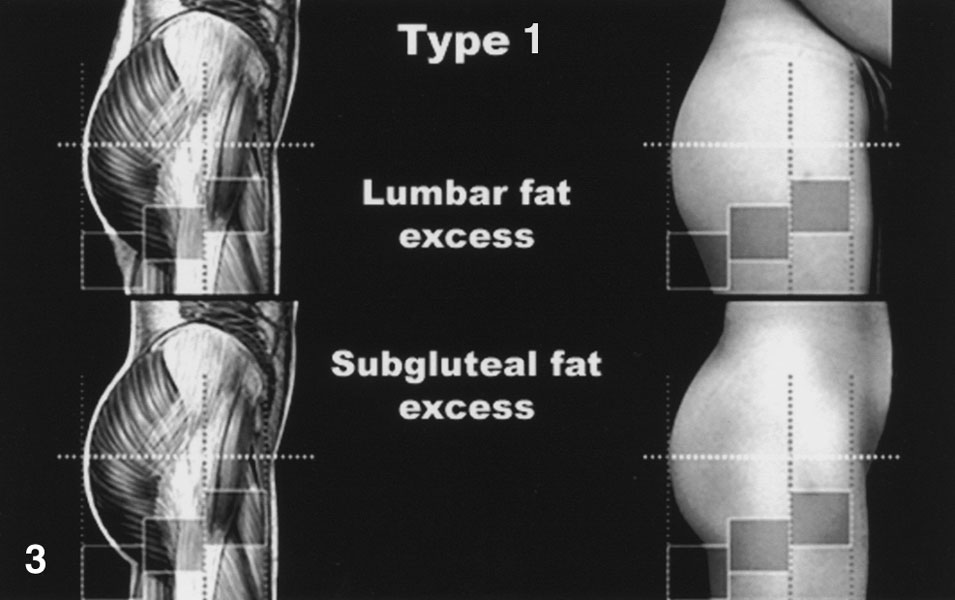
Figure 3. Type 1. AC:AB ratio 2:1 or greater. Excess perigluteal fat.
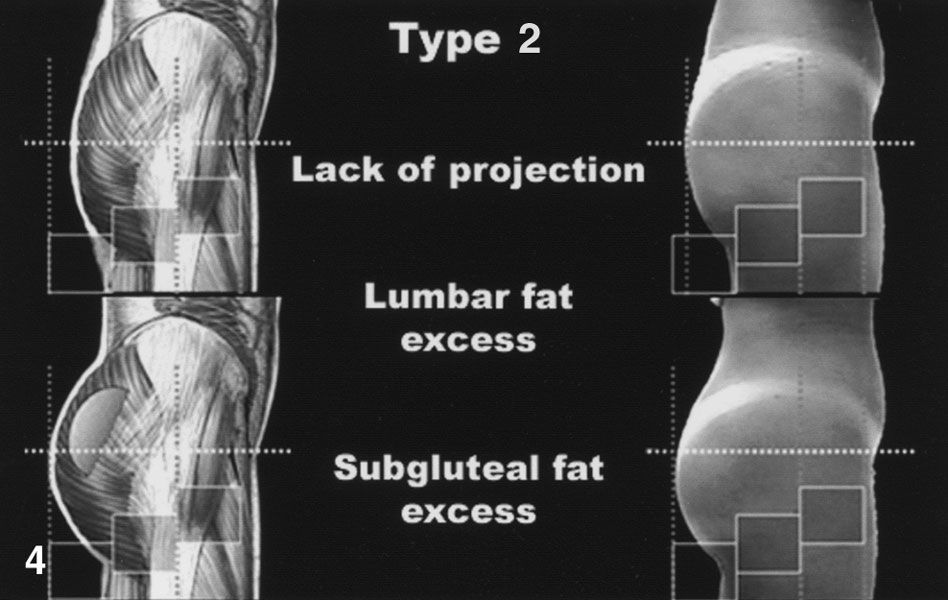
Figure 4.Type 2. Ratio lower than 2:1. Adequate volume, lack of projection.

Figure 5.Type 3. Ratio of 2:1 or greater. Lack of volume, usually with lumbar hyperlordosis.
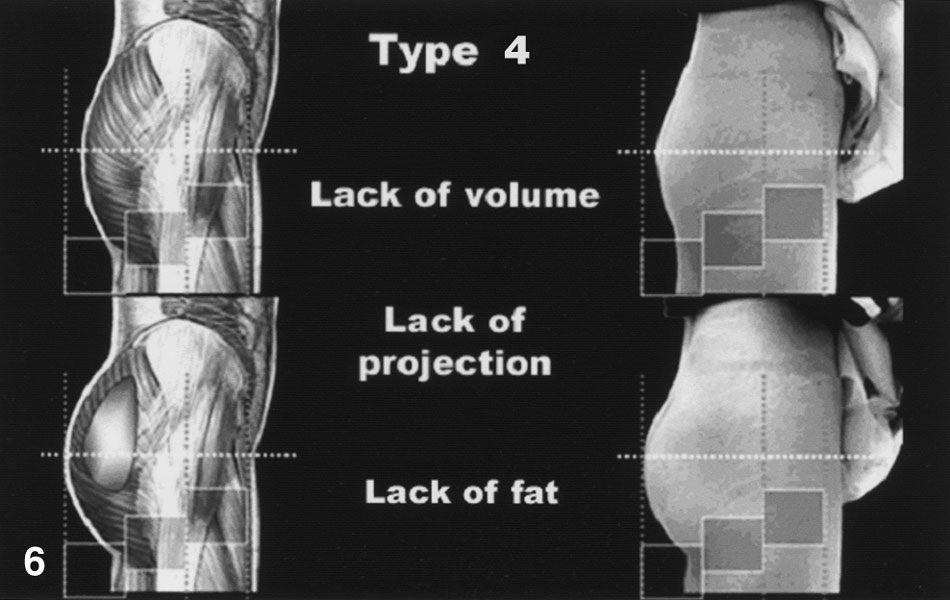
Figure 6. Type 4. Ratio lower than 2:1. Lack of anteroposterior and side-to-side projection attributable to a lack of volume.
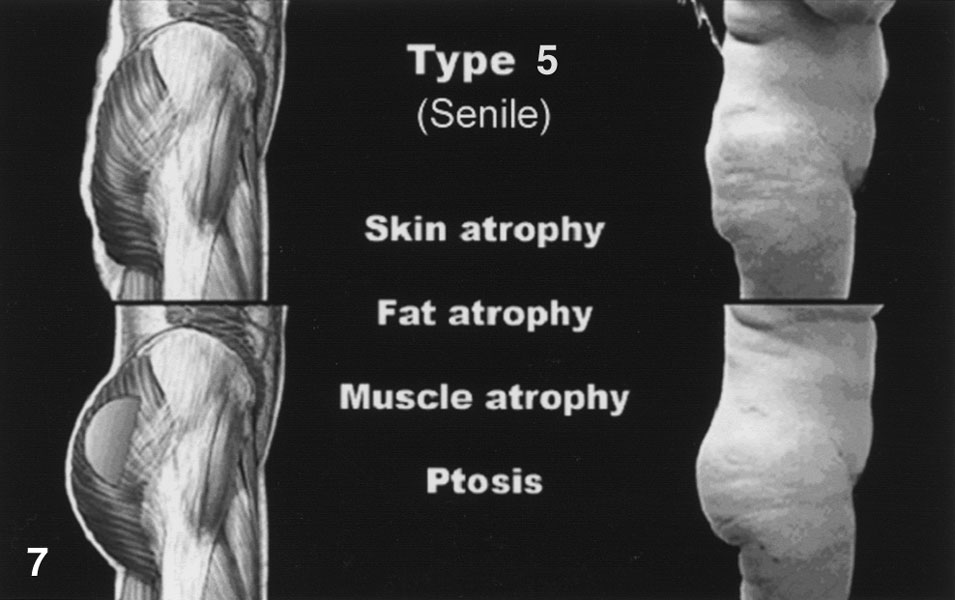
Figure 7. Type 5. Senile buttocks: hypotrophic, ptotic tissues.
Surgical Plan for the Various Types of Buttocks
Once these categories were established, it was possible to outline a treatment plan for each type of gluteal region:
Type 1
Because these women have acceptable projection and volume, with excess fat only in the paralumbar, supra-, and infragluteal regions, they can be managed solely with lumbar, supragluteal, and subgluteal liposuction, as well as liposuction in the trochanteric region [1]. Subgluteal liposuction to emphasize the fold may lead in time to gluteal ptosis, especially when it extends further than the median gluteal line.
Type 2
For these women, who have an adequate gluteal volume but little anteroposterior projection, we suggest using a round, small-based, high-profile gluteal implant (Robles design) [8]. This type of implant offers anteroposterior projection with no further side-to-side projection, which is achieved by the patient’s own gluteal volume. In addition, we perform liposuction in the areas of the buttocks that need it.
Type 3
For these women, lumbosacral hyperlordosis attributable to horizontalization of the sacrum simulates a large gluteal projection. However, there usually is a lack of gluteal volume, causing little side-to-side projection. Furthermore, the profile of the buttock makes a straight line with the thigh because of subgluteal lipodystrophy. To correct these defects, we use almond-shaped gluteal implants with a wide base and low profile (Otero design) [5]. These implants achieve a good side-to-side projection, but little anteroposterior projection. As in the preceding types, it is necessary to perform liposuction in the perigluteal region, emphasizing the infragluteal fold.
Type 4
For these women, we recommend a wide-based, high-profile implant (Vergara design) [9], which will achieve good side-to-side and anteroposterior projection. If any region shows lipodystrophy, liposuction also is performed.
Type 5
These women usually are in their fifties. All their body tissues, especially the buttocks, are hypotrophic and ptotic, with a lack of tone and turgescence. These defects cannot be corrected solely with the use of gluteal implants and liposuction. In most cases, it will be necessary to perform some type of wide dermocutaneous adjustment, a number of which have been published [3,6,7].
Surgical Technique
The surgical technique we use is based on the procedure described by Robles et al. [8], with some variations. The main difference lies in the preoperative planning and marking, starting with the patient in a standing position for the midline to be drawn (Fig. 8A). Next, the patient is asked to sit on the border of the examination table for the sitting line to be marked exactly where the buttocks rest on the flat surface. This line usually coincides with the greater axis of the piriformis muscle and is perpendicular to the midline (Fig. 8B). Then, 1 in. above, a parallel line is drawn as a safety zone, to avoid injury to the vessels and nerves, dissection should not extend below this line (Fig. 8C).
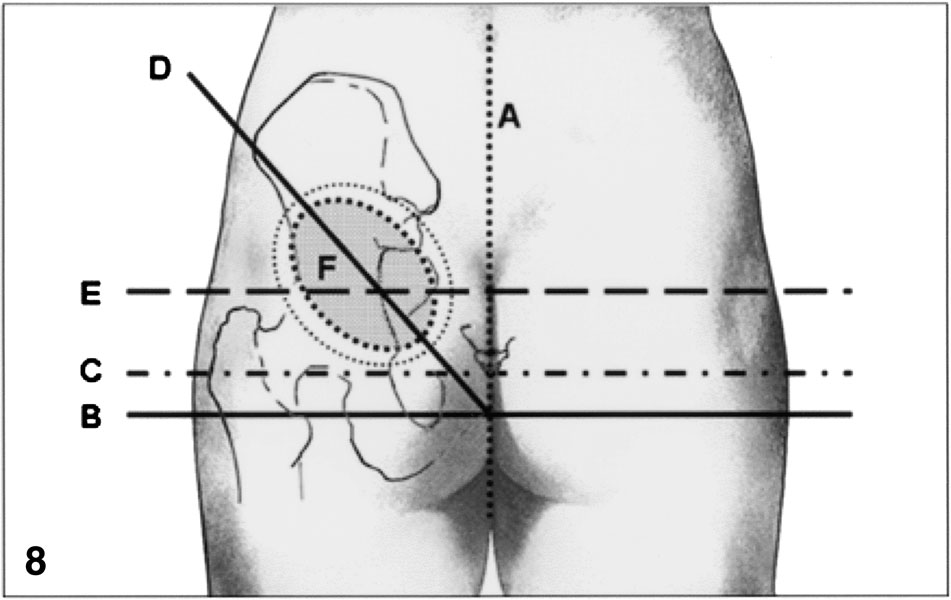
Figure 8. A, midline. B, sitting line. C, line of the safety zone. D, oblique lines from the anterior superior iliac spines to the coccyx. E, line over the point of maximal projection of the mons veneris, indicating the ideal point of maximal gluteal projection. F, outline of the implant's base plus margins for dissection. The point of maximal projection of the implant should be placed under the intersection of lines D and E.
Once these lines are drawn, the anterior superior iliac spines are located and two lines are drawn from them to the coccyx, meeting in the midline (Fig. 8D). With these oblique lines in place, we palpate the point of maximal projection of the mons veneris and draw a horizontal line perpendicular to the midline, crossing the two oblique lines. This is the ideal location for the point of maximal gluteal projection. It also should be the point of maximal implant projection (Fig. 8E).
As the final step in the surgical planning, the outline of the implants is drawn over the oblique lines, with care taken to make sure that the point of the implant’s maximal projection coincides with the ideal point of maximal buttock projection. If the implant is almond shaped, care should be taken to align its greater axis with the oblique line. Thus, it will have the same direction as the greater axis of the muscle belly. If the implant is round, the surgeon should watch only for the point of maximal projection.
We often mark an outline 2 to 3 cm outside the outline of implants which will serve as a guide for dissection (Fig. 8F). Once the area where the implant will be placed is marked, we outline the lipodystrophic areas (Fig. 9).
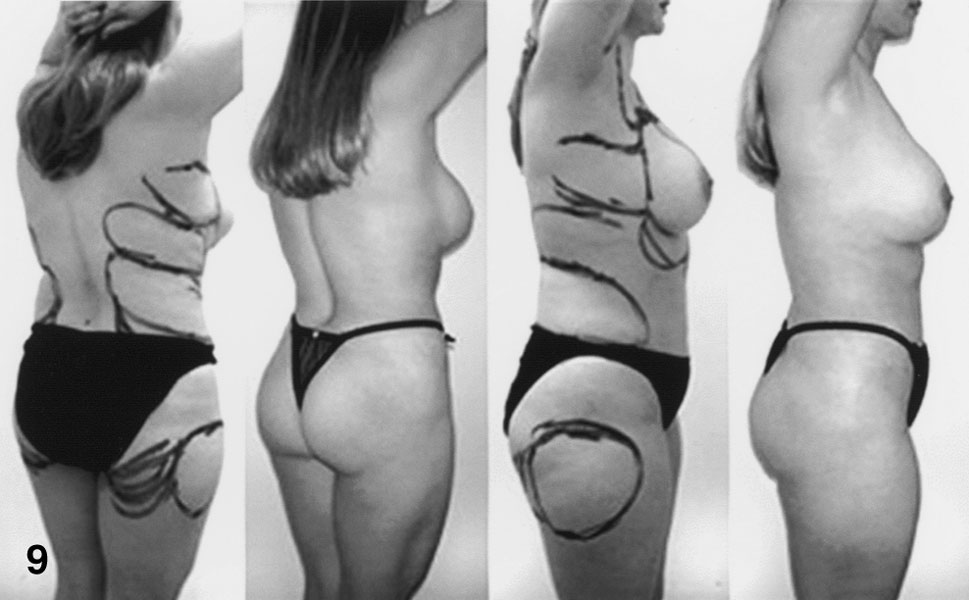
Figure 9. Marking of the areas for liposuction.
The patient is then placed in the face down position. The operation begins with liposuction of the areas previously outlined. Then, a 6- to 7-cm-long incision is made on the midline about 4 to 5 cm over the anus. The various planes are incised down to the deep layer of the superficial fascia, with care taken not to cut it because it lies immediately above the presacral fascia. Once this plane is reached, two incisions are marked, parallel to the midline and 1 to 2 cm apart, which will allow access to the right and left buttocks (Fig. 10).
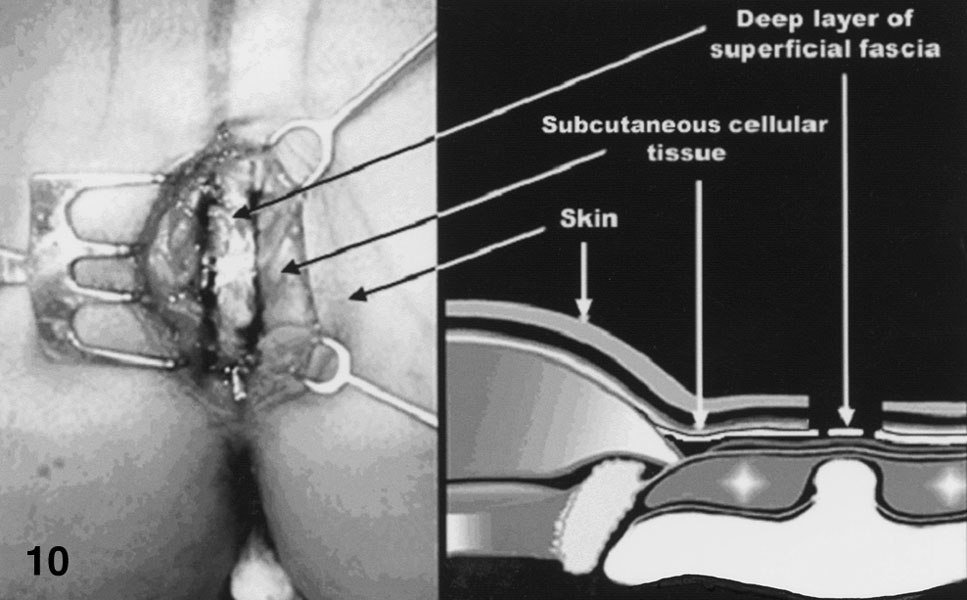
Figure 10. Dissection by planes down to the deep layer of the superficial fascia. Two incisions are marked parallel to the midline, 6 to 7 cm long and 1 to 2 cm apart, for entrance to the right and left buttocks.
To prevent injury to the presacral fascia and penetration to a deeper plane, dissection is performed carefully over the fascia right to the insertion of the gluteus maximus and 1 cm further into the muscle belly. The superficial fascia then is incised, and the muscle fibers are dissociated down to the deep fascia, with care taken not to create a cavity inside the muscle. The deep fascia is cut, and the dissection thus immediately reaches the subgluteal plane. Once in this plane, dissection is initially easy and bloodless, but upon arrival in the upper lateral quadrant of the gluteal region, it may become more difficult as the aponeurotic fibers of the gluteus maximus and gluteus medius are crossed. In the lower quadrants, dissection between the gluteus maximus and the piramidalis is quite difficult. To avoid injury to the neurovascular bundle, we perform no dissection in this area. Hemostasis is checked, and the implant is inserted (Fig. 11), with care taken to make sure that it is placed on the right axis and under the point of maximal projection.
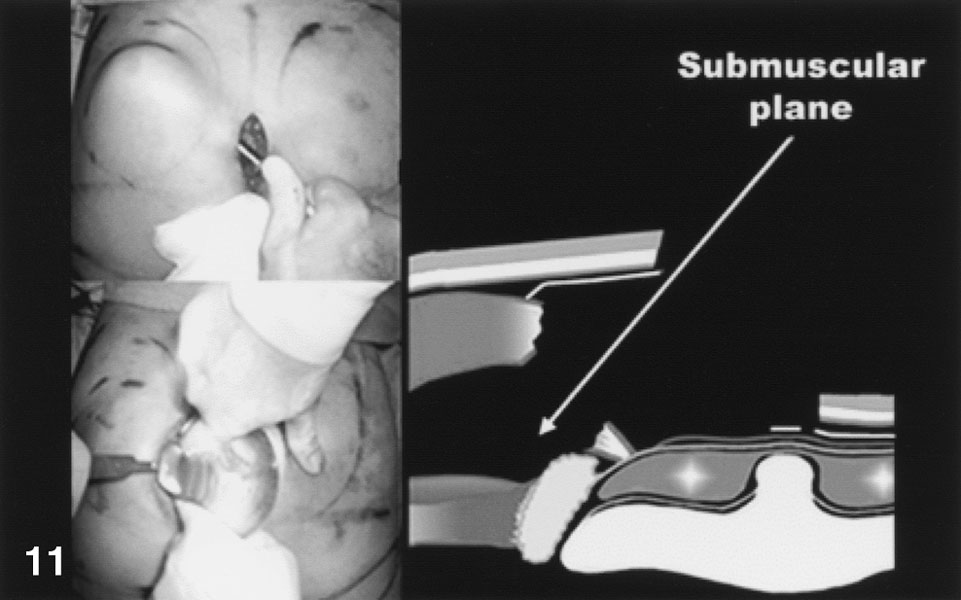
Figure 11. Dissection of the subgluteal cavity and placement of the implant.
Deep planes are closed with absorbable sutures. In suturing of the skin, full-thickness subdermal stitches are placed first, anchored to the edge of the presacral fascia between the two incisions made in it. This is done to sink the skin and simulate the gluteal crease (Fig. 12). Skin closure is finished with either interrupted stitches or a continuous intradermal suture, and the wound is sealed with collodion. The patient wears a girdle with gluteal openings for 4 to 6 weeks.
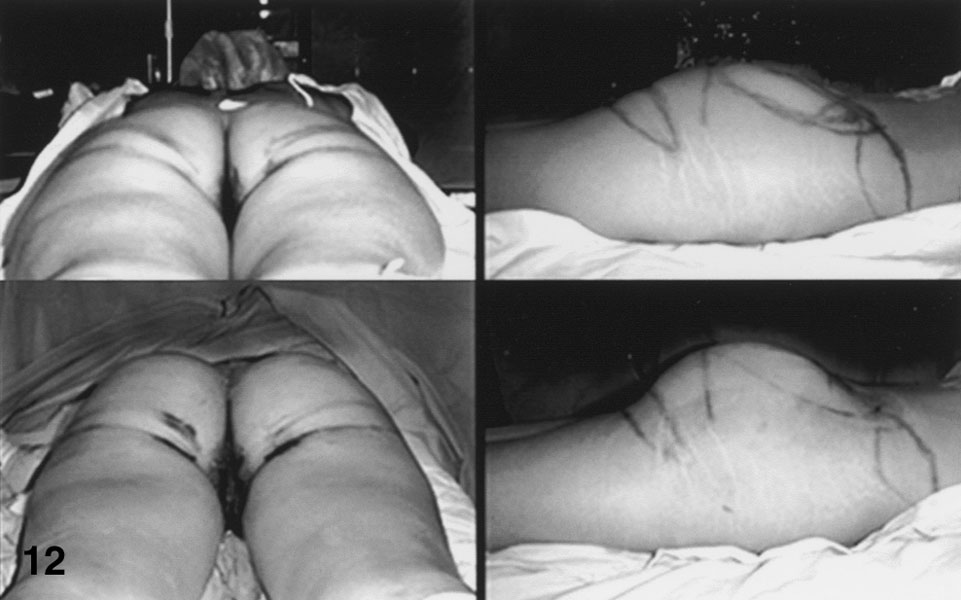
Figure 12. Dermal suture to emphasize the gluteal crease. Immediate pre- and postoperative views.
Discussion
To our knowledge, an aesthetic and anthropometric analysis of the gluteal region for surgical purposes has never been published. Thus, we consider our proposal a starting point from which other clinical investigators may modify or add to the measurements and other parameters. This set of suggestions is not intended to be a gold standard, but merely a guide for the decision to place gluteal implants, choose the adequate type, and determine whether liposuction should be performed and where.
Likewise, our classification for the various types of defects in this region is mainly for teaching purposes. Thus, when we speak of type 1 buttocks, we understand that the patient has adequate projection and volume, but that these are concealed by supragluteal, perilumbar, subgluteal, and sometimes trochanteric fat (Fig. 13). In these cases, liposuction may help to create a well-defined infragluteal fold, although it may involve the risk of eventually gluteal ptosis. By a type 2 patient, we mean a woman with an acceptable volume, but not enough projection (Fig. 14). When we describe in the medical record a female with type 3 buttocks, it means that the patient has enough anteroposterior projection, but little volume, leading to a lack of side-to-side projection, and that she usually has an ethnic or postural hyperlordosis (Fig. 15).
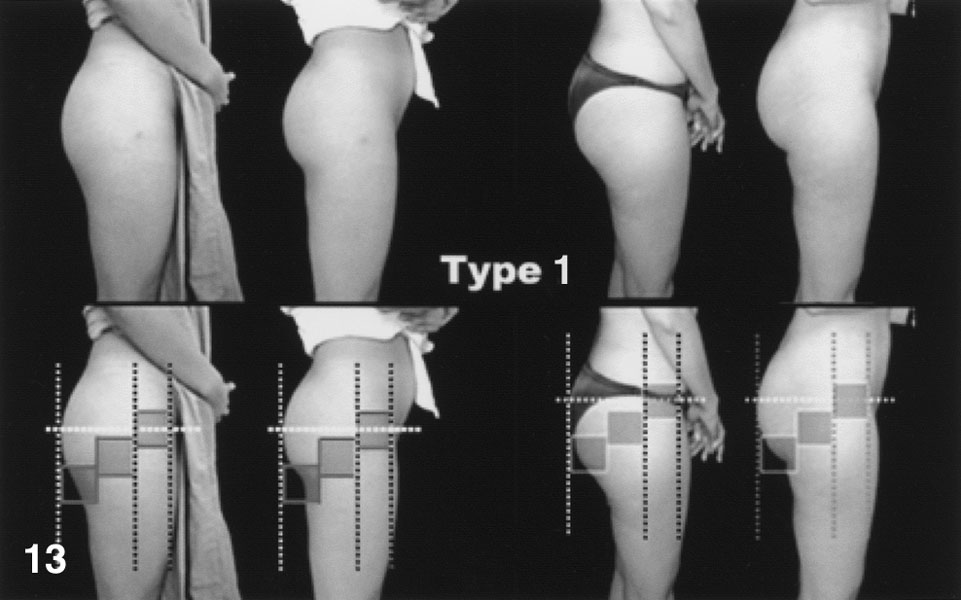
Figure 13. Type 1. Pre- and postoperative views. Only liposuction was performed.

Figure 14. Type 2. The preoperative view shows an adequate volume, with lack of projection and excess perigluteal fat. Postoperative view with round, high-profile prostheses.
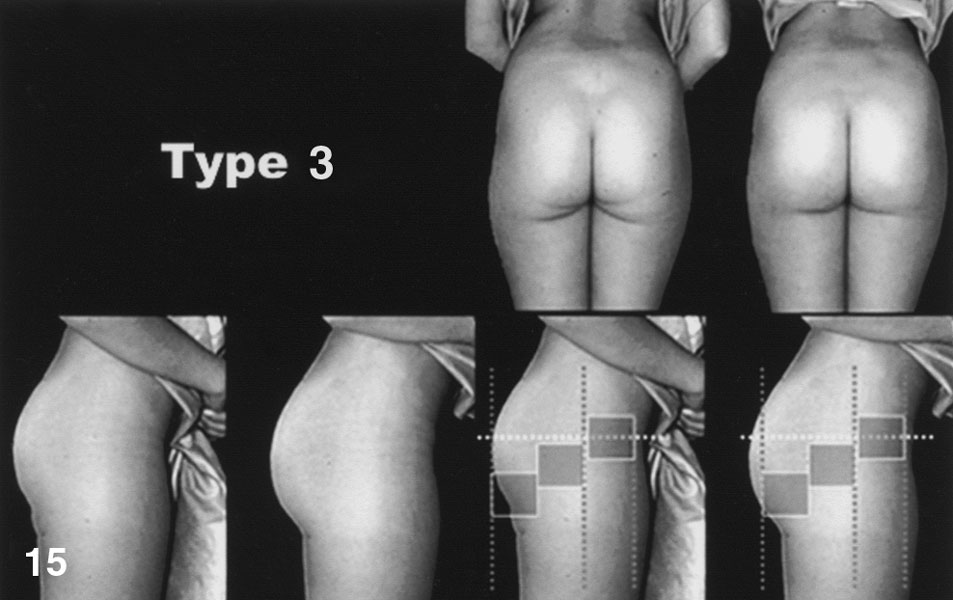
Figure 15. Type 3. Hyperlordosis, excess fat, and double infragluteal fold. Lack of anteroposterior and side-to-side projection. Wide-based, almond-shaped, low-profile prostheses were placed.
While the types help us to understand the kind of defect or defects, are they also a guide suggesting the surgical procedure that will allow us to correct them best. For instance, as soon as we identify a type 4 woman, thin, with an android pelvis and little anteroposterior and side-to-side projection, we are aware that we will need wide-based, almond-shaped, Vergara-type implants to achieve a good projection (Fig. 16).
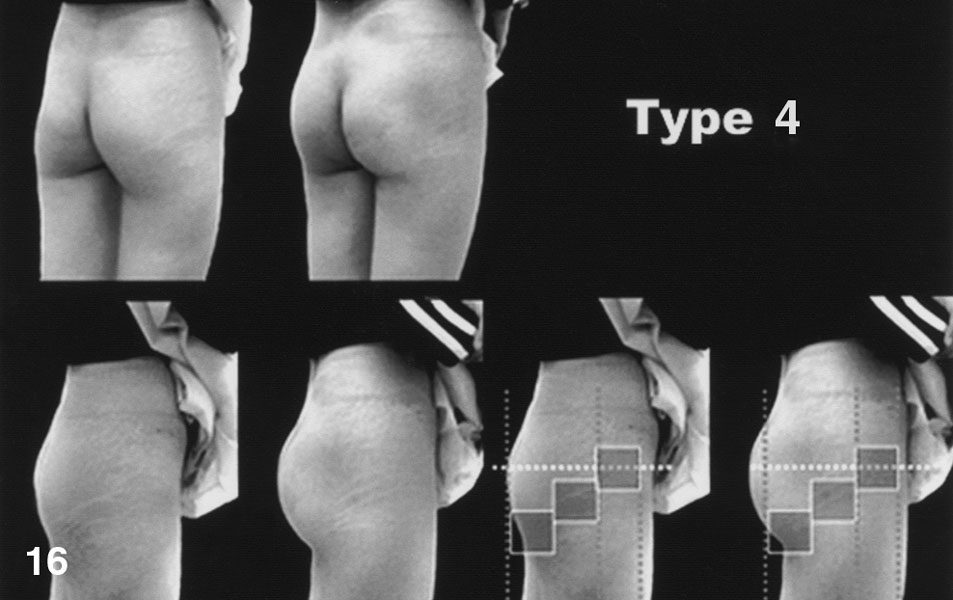
Figure 16. Type 4. No projection and no volume. Almond-shaped prostheses with a very wide base and a very high profile are necessary.
Finally, for a type 5 woman, we must plan for senile buttocks as well as wide dermal and fat adjustments, such as those described in literature, together with the placement of implants in case they are necessary (Fig. 17) [3,7,8].
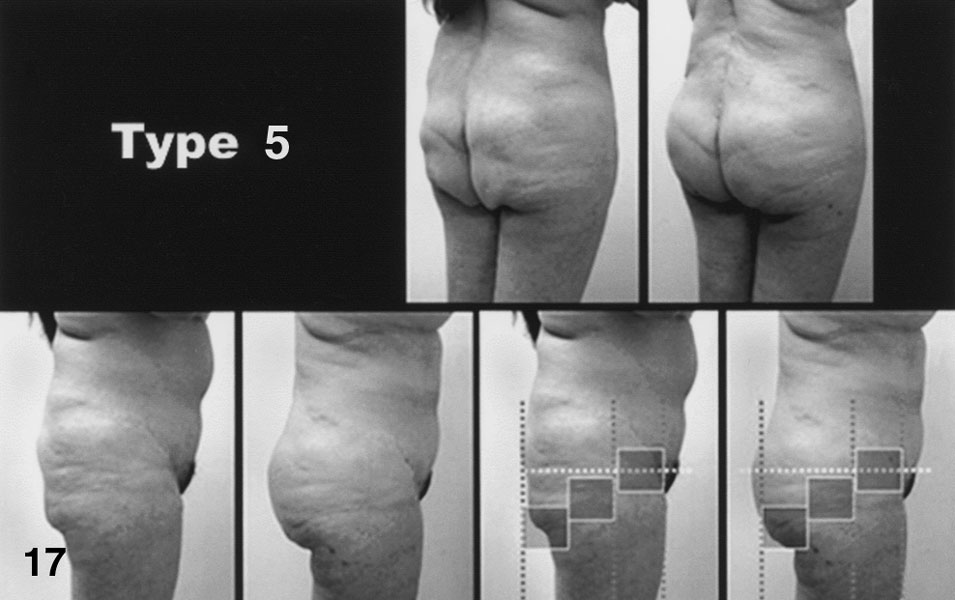
Figure 17. Type 5. Senile buttocks. A dermocutaneous adjustment is performed. High-profile implants with any shape are used.
This report aimed to define and describe defects in the buttocks by contrasting them with the features that give harmony and beauty to the gluteal region. This report is based on a wide series of photographs and a number of women. In contrast, a very small number of patients underwent surgery as sample cases for the surgical techniques suggested. Furthermore, as mentioned earlier, this is a proposal for the larger plastic surgery community to explore and either validate or reject.
The preoperative markings we use aim to facilitate safe and anatomic placement of the implants, with the maximal projection above the sitting line [2], and following the greater axis of the muscle belly (i.e., an oblique line from the anterior superior iliac spine to the coccyx) so we can create or emphasize the lateral depression of the buttocks, as well as the small V-shaped crease arising from the upper end of the gluteal crease.
There are several reasons for placing the implants in the submuscular space, as described by Robles et al. [8]. We believe it offers advantages that other spaces do not, such as an actual cavity among the gluteus maximus, gluteus medius, and piriformis muscles. Also, it is virtually bloodless because it is bounded by muscle fasciae, consequently making dissection easy, with no risk of injury to the muscles or neurovascular structures. Besides, it is easily approached from the gluteal crease. Nonetheless, its main disadvantage is the difficulty involved to reach the right plane.
The supragluteal space described by Gonzalez-Ulloa [2] has several drawbacks, such as ptosis of the implant, capsular contracture, malposition, seromas, and so on (Fig. 18), which often lead to removal of the implant. In the intragluteal space [9], the main drawback is the difficulty dissecting the whole gluteus maximus consistently and with a uniform thickness. Furthermore, irregularities in the cavity may be visible from the outside once the implant is in place (Fig. 19). Another disadvantage with this space is capillary hemorrhage that may start during dissection, complicate the procedure, and make it longer.
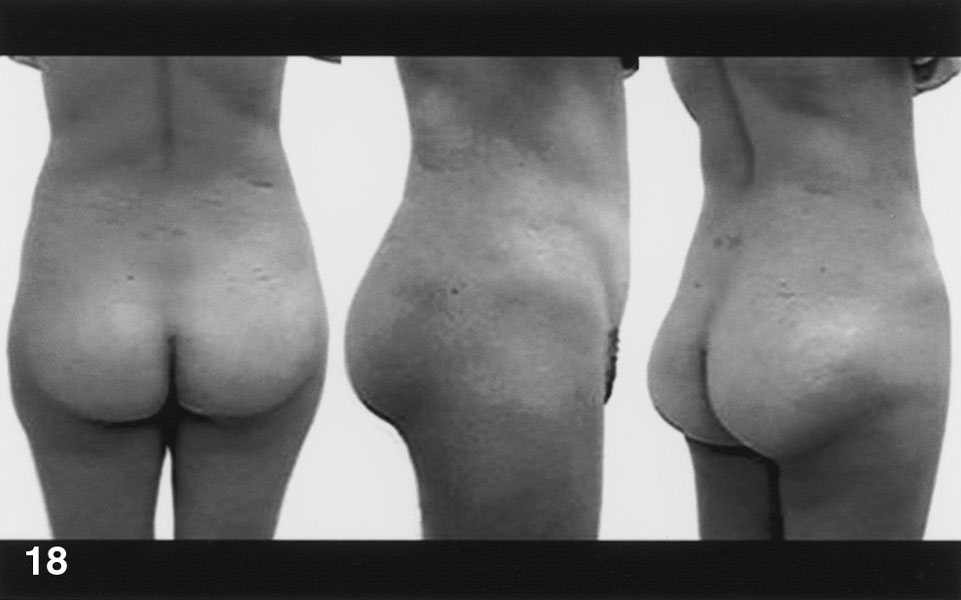
Figure 18. A 3-year postoperative view after placement of prostheses in the supragluteal space. Severe capsular contracture and ptosis of the implants have occurred.
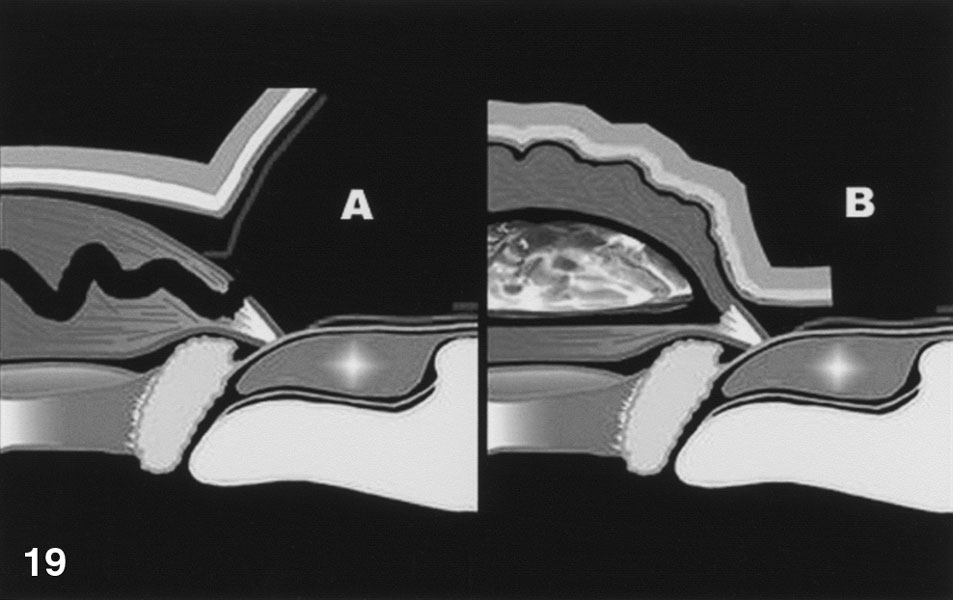
Figure 19. (A) Intragluteal dissection. (B) Once the prosthesis is in place, internal pressure makes ripples visible on the outside.
In summary, we consider that performing a systematic aesthetic and anthropometric analysis, taking into account the different types of deformities, using markings for the ideal location of implants, and using safe, accurate techniques for liposuction and placement of implants all will make it possible to achieve better postsurgical results that will lead to the well-being and satisfaction of patients.
References
- Cardenas-Camarena, L, Lacouture, A, Tobar-Losada, A (1999) "Combined gluteoplasty: liposuction and lipoinjection" Plast Reconstr Surg 104: 1524.
- Gonzalez-Ulloa, M (1979) "Torsoplasty" Aesth Plast Surg 3: 357.
- Lockwood, T (1991) "Transverse flank-thigh-buttock lift with superficial fascial suspension" Plast Reconstr Surg 87: 1019.
- Murray, M, Seireg, A, Scholtz, R (1967) "Center of gravity, center of pressure, and supportive forces during human activities" J App Physiol 23: 831.
- Otero, G (1990) "Gluteoplasty" Ann RAPS 5: 247.
- Pitanguy, I (1964) "Trocantheric lipodistrophy" Plast Reconstr Surg 34: 280.
- Regnault, P, Baroudi, R, da Silveira, C (1979) "Correction of lower limb lipodystrophy" Aesth Plast Surg 3: 233.
- Robles, J, Tagliapietra, J, Grandi, M (1984) "Gluteoplastia de aumento: implante submuscular" Cir Plast Iberolatinoamericana 4: 365.
- Vergara, R, Marcos, M (1996) "Intramuscular gluteal implants" Aesth Plast Surg 20: 259.
Comments
I have been going insane over the past 2 years about my wife's butt. It is not attractive to me and I can't get it out of my mind. I love her for all the other reasons, but I cannot have sex with her because she has a butt that is senile (as you described that type) and it is wider up high at the hips and tapers down. I hate that look.
I would to have her butt with more volumne toward the bottom (she has a lot of volumne off of her hips that is part of the problem from the full back view). Anyway my main problem is that I am in a dilemma. I keep thinking that if she gets surgery it will be phony. In other words it will not really be HER butt. So my choices are going crazy, finding an old photo of her where she had an acceptable butt (which I cannot find).remembering a good butt image of her in the past (which I cannot remember), or having her get a surgical procedure for volume and projective AND at the same time sort of feeling that the surgery is is not something that is phony and that it is really her. Is there ANY other more natural way to get volume and projection other than surgery. Is there any way to look at surgery as natural. For instance does her added fats work in conjunction with her natural body or is it just an add on?
HELP ME
Larry Robinson
Larry Robinson: Do it in missionary position or turn off the lights when doing it doggy style. Exercising the buttocks muscles will help add mass and improve looks. The quickest way to add muscle mass to the buttocks is to eccentrically challenge the muscles using specialized equipment. You may need to refer to a personal trainer for the know-how.
If your wife is older, then her backside likely looked better when she was young, and viewing surgical correction as a procedure that will be restoring more youthful looks should be less of a problem since she would be using it to acquire what she had rather than what she never had. Also, if you lean toward surgical correction, hopefully your wife should want it too; imposing it on her is not recommended.
Sweet halelujah you are so damn right. Why if I had my way the fairer sex would have a upper age limit, 30, like that film with whats his name. Then they would be piled into the back of a big 'ol pick up truck and dumped off the nearest cliff. Then, you could get another one, younger ya know, with nice titties and a tight ass, although you'd have to brainwash her into going anywhere near your wrinkly ol cock but hey, a mans gotta do what a mans gotta do right? Am I right? Eirk, imposing it on her is highly recommended! But your idea about electrocutin her ass is worth a go first. I have a big generator out back, and crocodile clips. Just bring her round larry! She wont know what hit her. I can put some nightol in her tea. When she wakes up she'll be able to bounce on it! Might put some life in your wizened old meat and 2 veg as well!!! And she'll no longer have to close her eyes and dream of Sean Connerey, one of the few men who get less physically repulsive with age!!!!!!!! Yeee hawwwwwwwwwww!!!!!!!!!!!!!!!!!!
good site
Very nice concept analysis and objectives. Keep it up
Very good read.. But whats up with all the advertisement comments.. unmonitored??
I fucking love you, Bob.
I've seen every ass on this cite and you have yet to post up a nice ass. All these flat asses on theis cite are not sexy at all. Even the ones you claim are rounder and more feminine. There is no ass on this cite!!!
You are seriously looking on this site for ass?
"but I cannot have sex with her because she has a butt that is senile".
This your problem, not hers. You are trying to make your wife get surgery to change her appearance so you can have sex with her. Please kill yourself now. You are a bad person.
Remember readers: look at the comment section of a non-forum site to find all the stupidest people in the world.